Endovascular coiling: A minimally invasive way to treat brain aneurysms
Finding out that you or a loved one has a brain aneurysm can be frightening. The good news is that many aneurysms can be treated without open brain surgery. One of the most common approaches is a procedure called endovascular coiling.
What is a brain aneurysm?
A brain aneurysm is a weak spot in the wall of a blood vessel in the brain. Over time, blood pressure can cause that weak spot to balloon outward.
Many aneurysms don’t rupture or cause symptoms. They may only be found by chance during imaging for another reason.
However, if an aneurysm ruptures, it becomes a medical emergency known as a subarachnoid hemorrhage – a type of stroke that can be fatal.
Symptoms include:
- A sudden, severe headache, often described as the worst headache of your life.
- Nausea and vomiting.
- Stiff neck.
- Loss of consciousness.
- Weakness.
- Vision problems.
What is endovascular coiling?
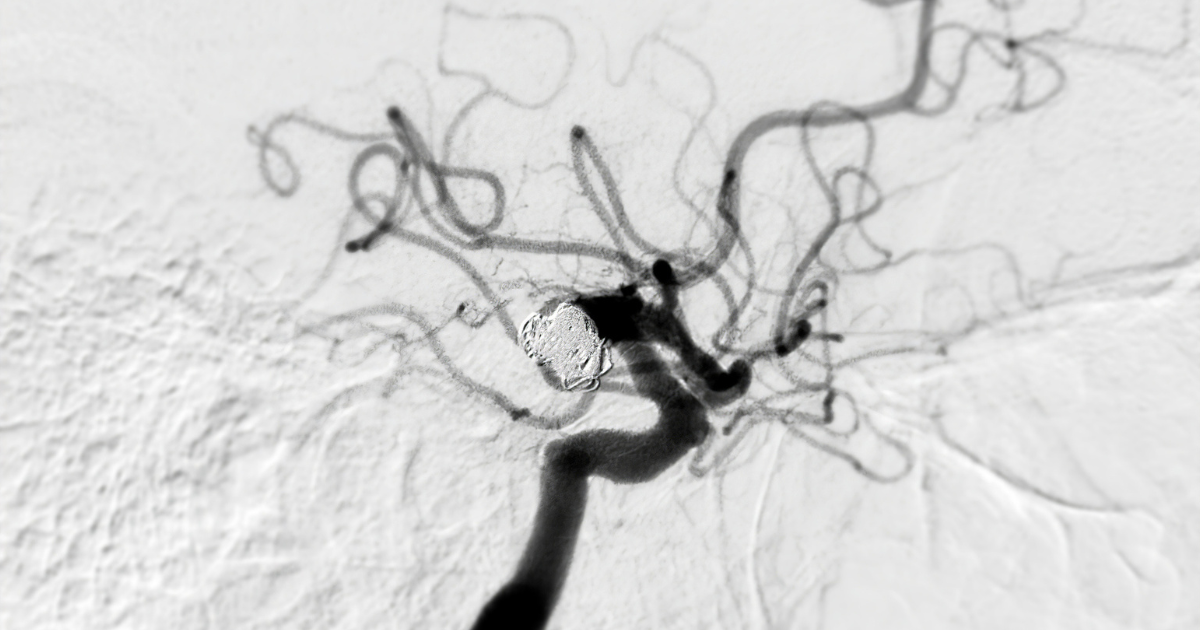
Endovascular coiling is a minimally invasive way to seal off an aneurysm from inside the blood vessel.
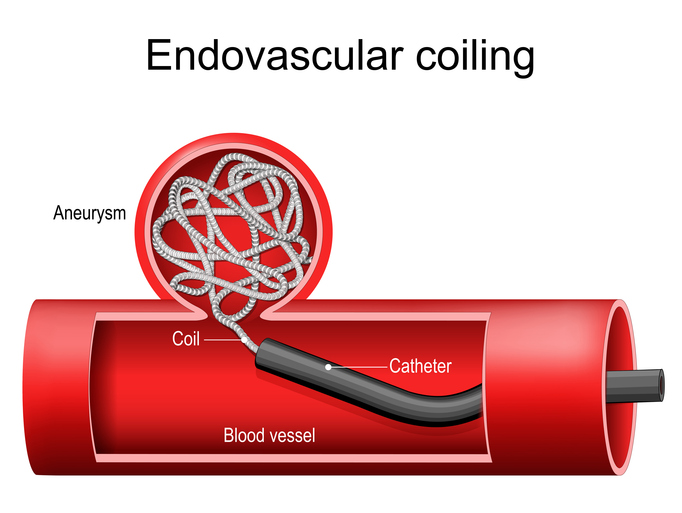
A neurosurgeon makes a small puncture – either at the wrist or the crease of the leg – and threads a thin, flexible tube called a catheter through the blood vessels up to the brain. Once the catheter reaches the aneurysm, tiny metal coils are placed inside it.
“Some of the coils are wound in a helix, like a slinky, and others are in three-dimensional shapes so that they look more like a ball or a sphere,” says neurosurgeon Daniel Surdell, MD.
The coils fill the space inside the aneurysm and block blood from flowing in. Over time, the body forms a clot around them, permanently sealing the aneurysm.
In some cases, surgeons use a device called a flow diverter to treat an aneurysm without needing to place coils directly into the aneurysm.
“It basically acts as a scaffolding along that inner wall of the vessel to allow it to heal across an aneurysm neck,” Dr. Surdell explains.
Flow diverters are especially helpful when treating an aneurysm that is larger, originates from the carotid artery and is located near the base of the skull.
Who is a good candidate for coiling?
Coiling works best when the aneurysm has a narrow opening or neck and a larger dome – a shape that helps the coils stay in place.
When this is not the case, several endovascular techniques can be used to help make the anatomy more favorable for treatment. One common device used to assist in embolizing an aneurysm with a wide neck is a stent.
Many patients choose coiling because it is less invasive than open surgery.
“You can usually go home the next day,” Dr. Surdell says. “You just have a little poke, a puncture either in the artery at your wrist or the artery in the crease of the leg.”
Still, coiling is not the right choice for everyone. Depending on the size, shape and location of the aneurysm – as well as the patient’s age, overall health and personal preferences – open surgery may offer a more durable solution.
The Nebraska Medicine neurosurgery team is experienced in both methods.
“We try to go into it with a very thoughtful approach,” Dr. Surdell says. “We have a discussion about our options and reach an agreement about what’s best for you.”
What are the risks?
If you have an unruptured aneurysm, your neurosurgeon will review all risks with you and help you understand how they compare to the risk of leaving the aneurysm untreated.
For patients who present with a ruptured aneurysm, also known as a subarachnoid hemorrhage, the situation is more urgent.
“In the case of subarachnoid hemorrhage, patients are very sick,” Dr. Surdell says. The care team focuses first on stabilizing the patient, managing fluid buildup in the brain (hydrocephalus) and preventing a second bleed with the most appropriate intervention.
What happens after coiling?
For patients who had a planned, non-emergency procedure, follow-up is typically straightforward. Imaging – usually a MR angiogram – is done around six months to one year. Another MR angiogram is often obtained again after one year. Patient-specific long-term follow-up is then established periodically after those initial studies.
Long-term follow-up matters.
“You can see recurrence of the aneurysm beyond five years, so sometimes five-year interval imaging is recommended,” Dr. Surdell says.
For patients hospitalized after a rupture, recovery involves two to three weeks of intensive monitoring for complications. These may include:
- Fluid buildup in the brain, also known as hydrocephalus.
- Changes in sodium levels.
- Vasospasm, a temporary narrowing of blood vessels in the brain caused by the breakdown of blood products.
- Seizure, or abnormal electrical activity in the brain.
Where can I get care?
Nebraska Medicine offers the region’s leading Joint Commission Certified Comprehensive Stroke Center. Patients with ruptured aneurysms receive care in Nebraska Medical Center’s dedicated Neuroscience Intensive Care Unit.
Dr. Surdell encourages anyone with a cerebrovascular issue to contact the neurosurgery team.
"Talk with us,” he says. “We're available to speak with patients directly, answer any questions and provide second opinions.”





